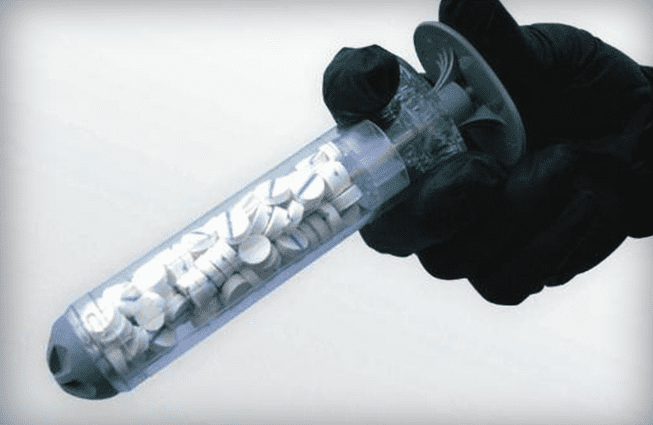
If you read Jon Wayne Taylor’s excellent series on gunshot wound first aid, you’ll probably remember rule number one of dealing with a hole: squeeze, squeeze, squeeze until the red blood stops. There is no substitute for pressure in stopping leakage. And while a tourniquet is usually the best way to stanch the flow, depending on the wound location, sometimes a tourniquet isn’t an option. Toward that end, RevMedx has developed a wound-plugging syringe, the Xstat, that’s meant to stop a thigh bleed kinda like you’d plug a hole in your tire . . .
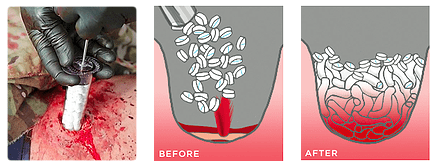
The syringe works by injecting small, expandable cellulose sponges into wounds that can’t be stopped from bleeding with the use of a tourniquet (e.g. wounds in the groin or armpit). The sponges expand on contact with blood in just 20 seconds, blocking its flow out of the body. Each applicator absorbs up to a pint of blood and up to three syringes can be used on a single patient.
The Xstat has just been approved by the FDA for civilian use. No word on cost yet, but this would seem to be a worthy addition to your blowout bag along with a SOF tourniquet, some quick clot and a hell of a lot of gauze.



I like this, but, functionally, how is it different than just shoving QuckClot gauze into a wound and packing it with my finger?
Or using a tampon ….
Tampons don’t have a chemical coagulant.
I’m a emt, +1 on the tampon! And tourniquets are great and all, but a few tampons and an isreali bandage would go allot farther in my opinion. As a side note, you could improvise an ashermans chest seal with a heavy duty party Balloon (by cutting the bottom off) and applying a judicious amount of crazy glue…just a thought…probably better to just buy the real thing…
Probably not much, but maybe less chance of getting your finger penetrated by a bone shard
Good point. Oddly enough I’ve never thought of that and with hundreds of patients, that never happened. I guess because I always had the gauze in front of my fingers, but it is something to consider. Thanks
Another reason would be that it can get it in deeper than your fingers can reach.
Could be more sanitary If it comes in a sterile case. Quick clot is great but such a pain to clean up and you may not have a way to clean that finger of yours as you don’t want to add risk of infection to a major wound right?
The older QuickClot material is a pain to clean up, but they’ve made a gauze impregnated with the stuff for a few years now. I used it extensively and it worked extremely well. Sterility really wasn’t ever an issue for me, as the penetrating trauma removed any chance of a sterile environment.
What happens when you use more than three?
Maybe it’s like crossing the streams.
Ok, this is basically heresay, but I’m going to do my best to forward knowledge gleaned from my wife, a bio-medical engineer whose job primarily consists of designing test methods for medical devices that will allow their products to be approved by the FDA.
In order for a medical device to be approved by the FDA it essentially has to pass two criteria: The device must be designed for application to a specific medical situation, and it must be proven to be significantly effective for treating the situation– for those with a little stats in their background, p < .05.
I am going to go out on a small limb and say this: Each syringe can absorb upwards of a pint of blood, if you remove 3 whole pints of blood from a person's system, they are now in the range of severe Hypovolemic Shock, aka you are bleeding to death.
When the makers of Xstat did their testing, they were probably unable to see any significant difference in a situation that required 4 or more of these syringes to stop a wound, basically I am figuring that if you have that many holes to plug up or you have a huge gaping wound, you will likely not be surviving without some immediate surgical care.
So, here's the thing though, once the product is out on the market, it can be used in any way that people see fit. A Corpsman in Afghanistan, an ER doctor in Chicago, an average joe that happens to have 5 of these on him when he gets shot in a drive-by, could plug holes up left and right with these things, but the liability shifts off of the medical device company when such off device use situations arise.
My wife likes to tell the story about a doctor who took twenty something of their devices, of which you are supposed to only use one of, and put them all in a patient to save his life. That doctor can do whatever he feels is necessary to save a patient, and he got in absolutely no trouble for doing so in this situation, but if he asked my wife's device company if he could do what he did with their products, their answer, legally, must be ,"Our product is not approved for this procedure."
It guess absorbs too much blood. If you need to use three, the victim will essentially bleed out into the pads instead of the ground. (I would also hazard to guess that the coagulant does not do good things to your bloodstream in general.)
NOTE: Not a doctor, so this is me guessing. Someone with some actual training should feel free to correct me, I would love to know.
That’s what’s in my jump bag, along with a combat TQ and some Israeli gauze.
This looks rather spendy.
The Israeli gauze, does that stuff have a shelf (or trunk) life?
As hot as trunks get…
Lasts for years, even in the trunk.
Israeli gauze, also known as a pressure bandage, does not have a shelf life as it does not have any chemicals in it. Quick Clot, or combat gauze, does have a shelf life of about five years as the hemostatic agent does degrade over time. Army Combat Medic in case you were wondering about my credentials.
I’m excited for this since I think it’s probably easier for morons like me. I have received a short briefing on packing a wound with gauze, but this would seem to be almost idiot proof. Though I think the uninitiated may not realize you’ll have to push it in the wound to make it work.
That photo…just…ouch. I wouldn’t say I’m squeamish, but I’m actually feeling a bit ill right now. Still, alive is better than dead, and if this thing works…
Glad I’m not the only one, that thing creeps me out.
Better than bleeding to death or going through a TSA checkpoint though
My first thought was, “Ew! Ew! Ew!” This story gave me the heebiest of geebies!
Mine was “Holy, crap! That’s gonna *hurt*!”
Then again, the dead don’t feel pain…
You should see the other guy..
Add it to you bag right next to your Stimpacks and Rad-a-way
LOL!
+111
For the Fallout reference
This was my first thought after seeing the name!
+101
Nice. Kicking it old school.
+13.
Simple devices that can be used to stop deep penetrating trauma is are extremely valuable. I’d like to get my hands on a couple of these to try them out.
How would you go about trying them out? (genuinely curious, not trying to be a smarta**) What kind of trials could you put them through?
Stick them in something bleeding and note the result.
Shoot a hog, then treat the wound? Didn’t the Army used to use pigs as human analogs for treating bullet wounds? Before it became politically incorrect to give our troops proper training and RoE.
The US Army used both goats and pigs for testing terminal ballistic efficacy. The first board was “the goat board,” then there were objections that goats don’t simulate humans that well, so they re-did the research with pigs, which was informally named “the pig board.”
It didn’t matter – the findings were ignored anyway and the .30-06 was chosen for reasons of logistics.
DG, live animal tissue labs are still common practice.
The Army still uses pigs to train Combat Medics on how to treat battlefield injuries. Usually what they end up doing is the same group testing out new weapons conducts their test and then the medics go in to try to save them, while the pig gets shot/blown up again until it dies.
Forget about it unless you have a friendly doctor on retainer. Right at the top of the product description page you’ll find this:
CAUTION: Federal law restricts this device to sale by or on the order of a physician
Mr. Zimmerman says it “has just been approved by the FDA for civilian use.”
Maybe it was Rx only before, and now they can remove that restriction.
Black market.
I have CELOX-A and CELOX granuals in my blowout kit.
There are places on the body where you’re not supposed to use Quick Clot because it can get into the bloodstream and clot in other places, like the heart and lungs. It sounds like this wouldn’t have this problem so it could be used anywhere on the body that’s wide enough for the syringe to be applied.
Man, that just looks like it’ll hurt like hell. If I ever have to have one of those used on me forget macho. I’m gonna scream like a little girl.
Hopefully I’ll pass out and won’t come around til the recovery room or the pearly gates.
jwm – “Phew. Well, I died! That was rough. Don’t let anyone tell you dying’s easy. But I got through it! Wait… What’s that up ahead? The Pearly Gates? Cool! Is that St. Peter I see? Doesn’t look like him… Oh, no! That’s not St Peter! That’s Hillary Clinton! This ain’t Heaven! I’m in HELL!”
[The Trap Door opens…]
🙂
Hell would be a naked hillary waiting with a leash and dog collar.
…and a strap on.
Well the alternative ain’t much better. Meaning someone shoving gauze in there with their finger.
I mean bleeding out isn’t a walk in the park, either, though perhaps it hurts less. ;p
the proper term for using a product in a way not approved by the FDA is called “off label use”
A lot of our routine ways of doing things in Anesthesia constitute off label use
In Anesthesia, I usually transfuse anyone who loses 30% of their estimated blood volume during surgery.
The average adult male has a blood volume of 5,000cc
5,000cc x 30% = 1,500cc
Since a pint is 473 cc, lets use 500 cc to make the math easier
3 pints is 500cc x 3 =1,500cc
I would insist on transfusing any adult male who lost 1,500 cc of blood during surgery.
Using three of these devices means the patient now needs a blood transfusion
How do you get it out without going to a hospital?
You don’t. It needs to be surgically removed. If you need this, you need a hospital, probably a level 1 trauma center.
Good, nice, but wouldn’t it be better to just retain the pelletized material in a semi-rigid “wringable mesh” sleeve that can be ‘wrung-out’ internally (and internal to it’s own permeable housing) with a gentle twist before removing?
The ‘insert’ could expand under the expansion of the absorbable internal material, but could be made to absorb/filter excess fluids [with an internal (to the device) semi-flexible aspirator pick-up straw]. It would seem to make wound clean up much easier.
There could also be coatings that indicated sepsis onset, gangrene, chemical/biological/radiological/magnesium-phosphorus exposure indicators, etc.
You’re looking at treatment too far down the road. I believe the point of these is to get the patient from the place where he was wounded to the hospital, without him bleeding out. Then the hospital would send him into surgery immediately, remove the clotting material, and repair the wound. It’s an emergency first aid tool, not a long-term solution.
It can be nearly the same device, used in the same way, but what I wrote would make the removal easier and would allow for the instrument to do other things as well.
I WILL get me a couple of these for my kit.
I thought these were a great idea when I first read about them.
I remember seeing a video on this. Supposedly, it has led to a dramatic increase in survivability on the battlefield. It is supposed to be significantly more effective and quicker to apply than packing a deep wound with gauze.
With all due respect, I’m awaiting the hospital case horror stories of people using this up their butt for literal shats’n’giggles gone horribly wrong now that it’s available to the public.
Comments are closed.